Bladder pain syndrome: differences in diagnostic strategies around the world
1 University of Pennsylvania, Philadelphia, United States
Abstract
Nomenclature for the syndrome commonly referred to as bladder pain syndrome is in flux. In the United States the disorder is interstitial cystitis/bladder pain syndrome reflecting one entity. This reflects the need to keep the term interstitial cystitis for health insurance purposes. In Europe bladder pain syndrome is now the well-accepted nomenclature. In Asia, the situation in more complex. The terms frequency/urgency syndrome, hypersensitive bladder syndrome, painful bladder syndrome, and interstitial cystitis all carry different connotations and overlap to some extent.
A presumptive diagnosis requires a history compatible with the definition of symptoms, a physical examination, urinalysis, and exclusion of any confusable diseases. This is a major area of harmonization around the world. Further evaluation with cystoscopy and hydrodistention of the bladder is commonly done in Europe and Asia at the time of initial diagnosis, but is not considered mandatory.
To further harmonize nomenclature, diagnosis, and treatment algorithms and enable international clinical research to improve therapies, the International Consultation on Incontinence recently organized a meeting in Tokyo, hosted by the International Continence Society meeting Sept. 2016, and a further meeting, the International Consultation on Interstitial Cystitis Japan is planned in April 2018 in Kyoto.
Summary of recommendations and introduction
Bladder pain syndrome, formerly referred to as “interstitial cystitis” is now defined and diagnosed in such a way that it can no longer be considered a rare disease. It may affect up to 2.7% [1] of the adult female population and the prevalence in men may approach that in women, at least in the United States [2]. The last 25 years have seen a worldwide effort to try to standardize its nomenclature, definition, and diagnostic algorithm [3]. While there has been significant harmonization that facilitates clinical research and pharmacologic trials, there is still a way to go and significant differences in approach remain. In this section we shall discuss nomenclature, diagnosis, and treatment algorithms in the United States, Europe, and Asia. Concepts are rapidly changing and international meetings occur virtually every year which make this really a snapshot in time of a moving target. At this time harmonization has been reached on the understanding that no invasive diagnostic studies are necessary to begin empiric therapy anywhere in the world. However, common practices tend to vary with the least invasive approach in North America and most invasive in Asia at this time.
Methods
A systematic literature search was performed for the last 10 years in MEDLINE with the following key words: bladder pain syndrome, interstitial cystitis, diagnosis, guidelines. Guidelines on management of bladder pain syndrome from the United States, Europe, and Asia were reviewed along with manuscripts detailing diagnostic methodology and approach to the syndrome. Relevant manuscripts are sited in the bibliography. Conclusions on the common practices and degree of harmonization were then formulated.
United States
The idea of a comprehensive guideline for what was then termed “interstitial cystitis” was initially approached in 1997. The American Urological Association (AUA) conducted a major literature review and abstracted all pertinent publications and held several meetings devoted to the topic. It was determined there was not enough scholarly material extant to develop a set of guidelines and the issue lay dormant for 10 years. A follow-up review was then undertaken and a database of publications from 1983 through 2009 yielded the material that formed the basis for the report [4]. The systematic review revealed insufficient publications to address IC/BPS diagnosis and overall management from an evidence basis. The guideline in these areas is purely grounded on expert opinion and consensus obtained by a Delphi technique [5]. Treatment (not a part of this section) was addressed on the basis of 86 treatment articles that met the criteria for value and evidence.
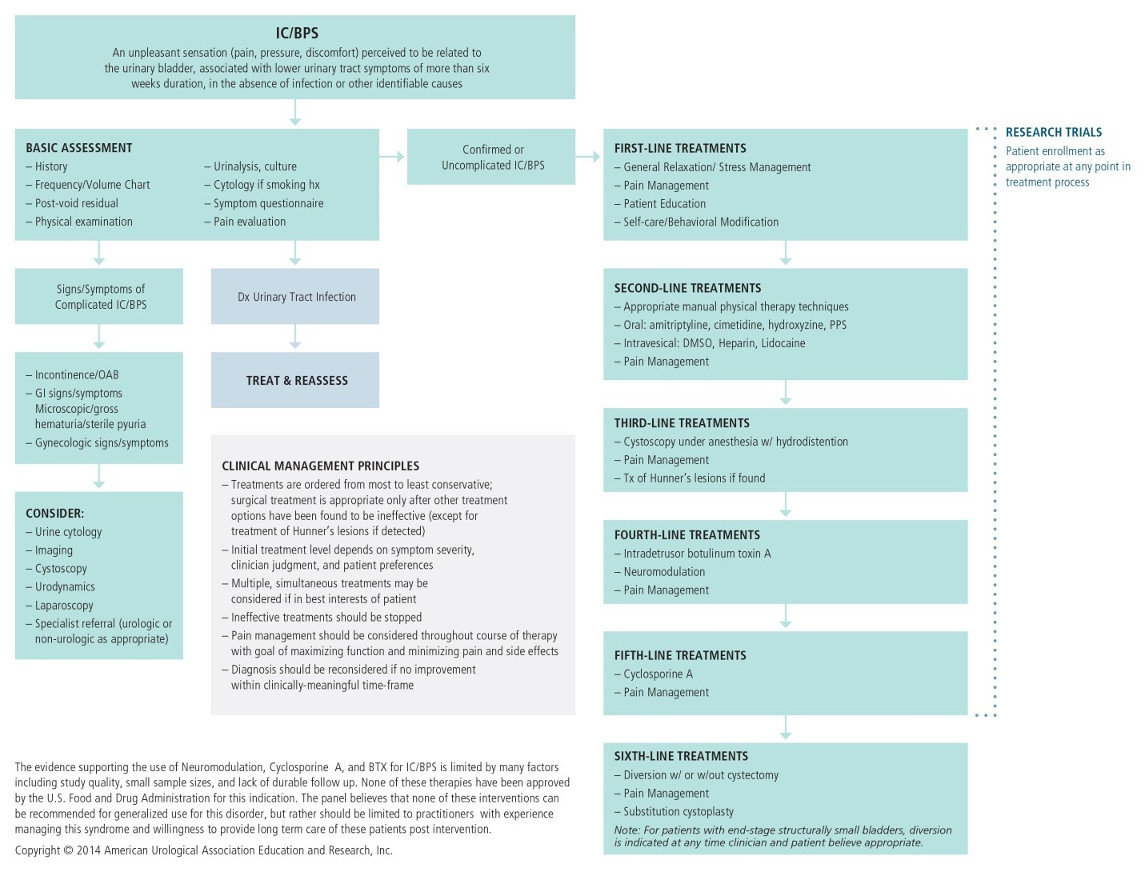
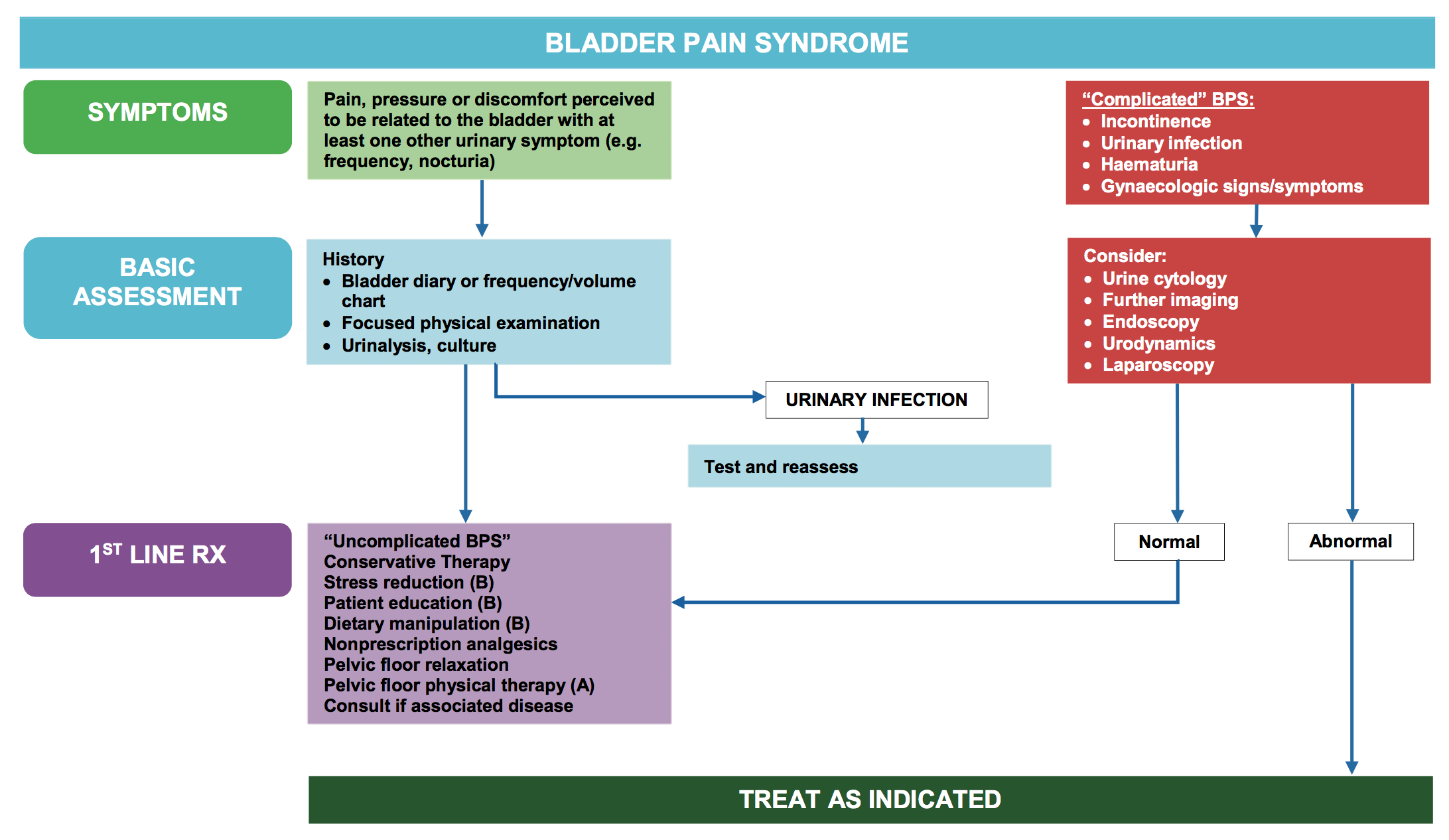
The guideline defined IC/BPS as a single entity and based the definition on the definition of the Society for Urodynamics and Female Urology [6]. “An unpleasant sensation (pain, pressure, discomfort) perceived to be related to the urinary bladder, associated with lower urinary tract symptoms of more than six weeks duration, in the absence of infection or other identifiable causes.” The definition allows treatment to begin after a relatively short symptomatic period, minimizing the delay in initiation of treatment which could occur with definitions that require longer symptom durations (i.e. 6 months). Definitions used in research or clinical trial should be avoided in clinical practice; many patients may be misdiagnosed or have delays in diagnosis and treatment if these criteria are used [7].
The prototypical IC/BPS patient may also present with urinary urgency and frequency, but these symptoms alone do not distinguish the IC/BPS patient from other lower urinary tract disorders. They must exist in conjunction with pain, pressure, or discomfort for the diagnosis to be entertained in the United States. The guideline goes on to state that the urgency experienced in the IC/BPS syndrome is more likely a function of pain than the fear of incontinence that is the hallmark of frequency from overactive bladder [8], [9].
Chronic prostatitis/chronic pelvic pain syndrome (CP/CPPS) in men (NIH type 3 nonbacterial prostatitis) can be difficult to differentiate from IC/BPS. It is characterized by pain in the perineum, suprapubic region, testicles or tip of the penis. The pain is often exacerbated by urination or ejaculation. While voiding symptoms such as sense of incomplete bladder emptying and urinary frequency are also commonly reported, pain is the primary defining characteristic of CP/CPPS. The AUA guideline notes that the diagnosis of IC/BPS should be strongly considered in men with pain, pressure or discomfort perceived to be related to the bladder when associated with frequency, nocturia, or urgent desire to void. The definition does not change for men, and indeed when applied it shows similar prevalence in men and women [2].
Insufficient literature was identified to constitute an evidence base for diagnosis of IC/BPS in clinical practice. The guideline recommends the following:
- The basic assessment should include a careful history, physical examination and laboratory examination to document symptoms and signs that characterize IC/BPS and exclude other disorders commonly associated with IC/BPS in the differential. This includes urinalysis, urine culture, standard evaluation with imaging and endoscopy for unevaluated microhematuria, and urinary cytology in those with risk of bladder cancer. The potassium sensitivity test [10] is NOT recommended because of poor specificity and sensitivity and the pain associated with the procedure [11].
- Baseline voiding symptoms and pain levels should be obtained in order to measure subsequent treatment effects.
- Cystoscopy and/or urodynamics should be considered when the diagnosis is in doubt: these tests are NOT necessary for making the diagnosis in uncomplicated presentations. The only consistent cystoscopic finding that leads to a diagnosis of IC/BPS is that of one or more inflammatory appearing lesions as initially described by Hunner [12]. Years before Wennevik’s landmark paper, the American guideline dismissed the significance of the presence or absence of glomerulations on endoscopy [13].
In a follow-up amendment to the guideline published in 2015 and incorporating literature through July 2013, there was nothing in the literature to call forth a change in any of the statements related to diagnosis [14].
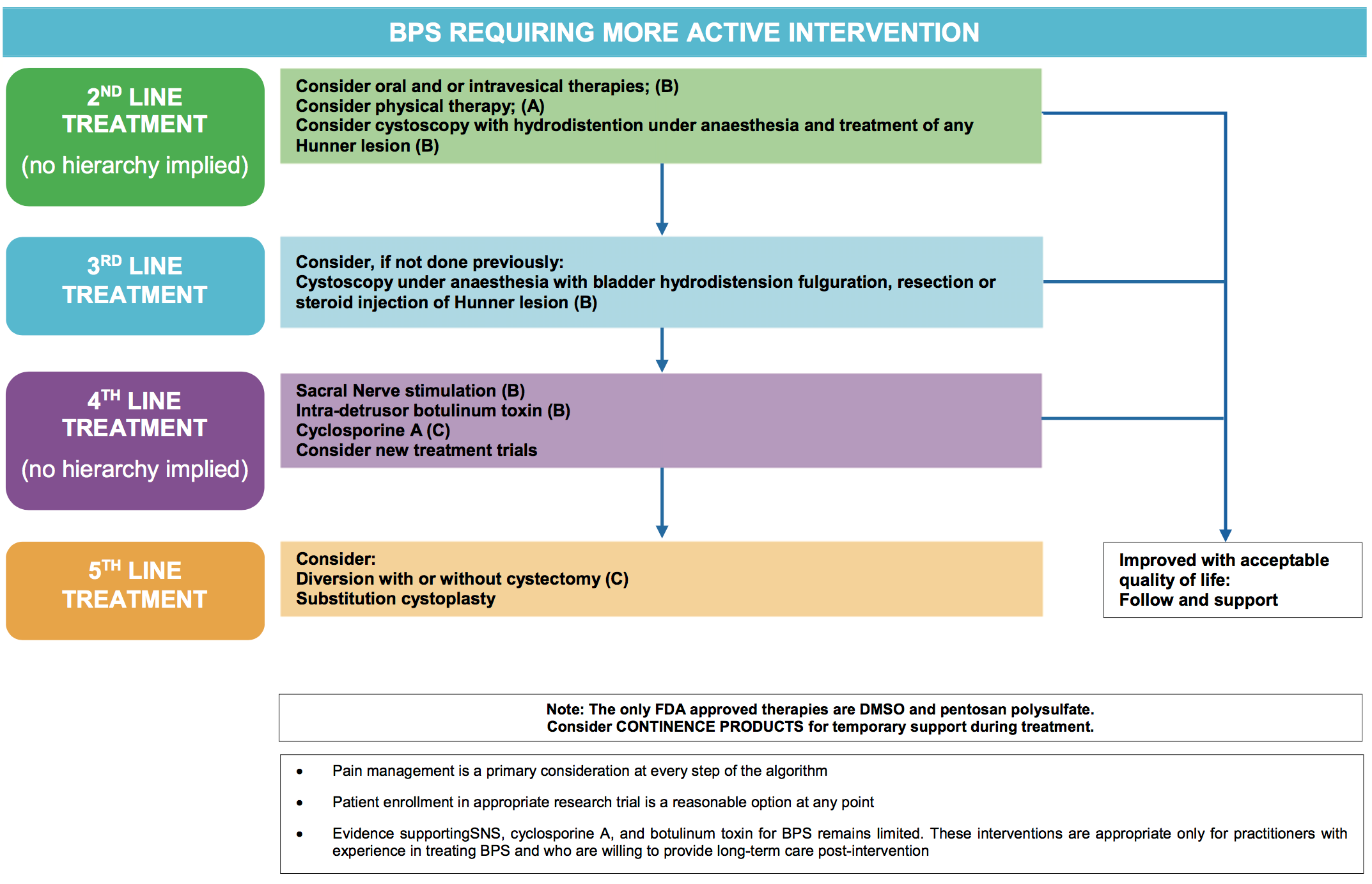
The definition, diagnosis, and treatment algorithm of the American Urological Association is reproduced as figure 1.
Europe
In Europe, the International Association for the Study of Bladder Pain Syndrome (ESSIC), initially a European group of experts from around the continent, has been extremely influential in formulating the definition, classification, and diagnostic strategies for this symptom complex. The group was formed by its first president, Jørgen Nordling [15], after the need for such a consensus building organization was demonstrated by the many different interpretations of bladder pain syndrome at a major international meeting in March 2003 sponsored by Dr. Tomohiro Ueda in Kyoto with expert opinions from 5 continents represented [16].
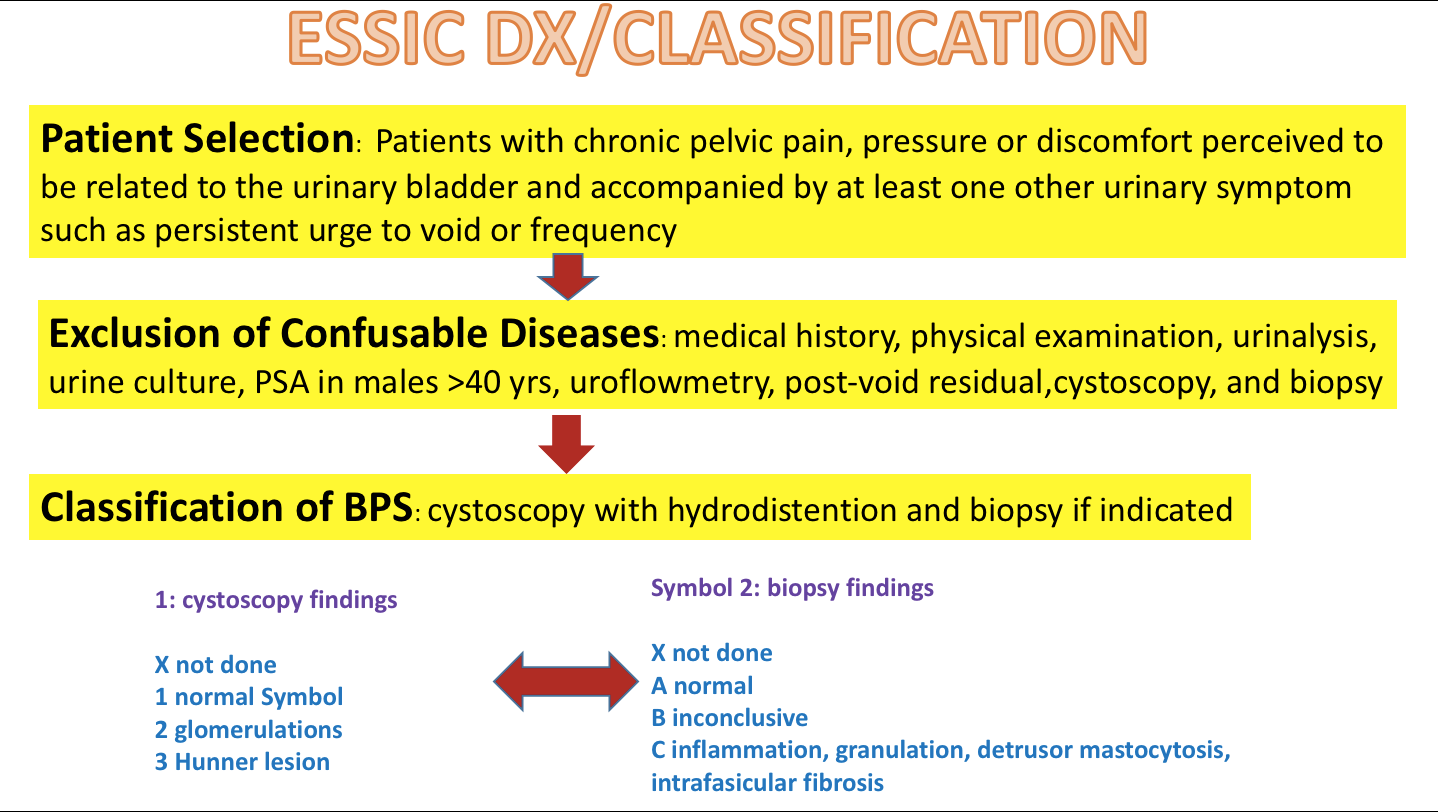
ESSIC proposed to give the syndrome, previously referred to as interstitial cystitis or painful bladder syndrome [17], a new name that would better fit into existing pain taxonomy [18]. This would also allow enable a unique definition, and thus minimize confusion. Bladder pain syndrome (BPS) was defined on the basis of chronic pelvic pain, pressure or discomfort perceived to be related to the urinary bladder accompanied by at least one other urinary symptom, like persistent urge to void or urinary frequency. Confusable diseases as the cause of the symptoms must be excluded. Further documentation and classification of BPS might be performed according to findings at cystoscopy with hydrodistention and the morphological findings from bladder biopsy. The presence of other organ symptoms as well as cognitive, behavioural, emotional and sexual symptoms should be addressed.
The ESSIC definition is based solely on symptoms. A six-month duration of symptoms was chosen for diagnosis, thus indicating that the condition had become chronic and would be unlikely to spontaneously resolve. A long list of confusable diseases and techniques to rule them out with appropriate testing is suggested, but it is left up to the provider to determine which confusable diseases are likely enough in a given patient to warrant further investigation. The jewel of the ESSIC approach is the classification system based on whether or not an endoscopic examination was performed and if so, whether tissue for pathological examination was obtained (figure 2). The presence or absence of endoscopy, glomerulations, and Hunner lesion provide for 8 categories, enabling patients with the syndrome to be studied within their cohorts to gather epidemiologic and treatment data. Patient in the 3X, 3B and 3C categories comprise the classic phenotype with Hunner lesions. Recent data indicating the lack of specificity, sensitivity, and prognostic values of glomerulations, nicely summarized by Wennevik, suggest that category 2 may be eliminated in future iterations of classification [13].
While the European Association of Urology closely follows the ESSIC, their definition of BPS as published in the guideline hews more closely to that of the International Continence Society: “Suprapubic pain is related to bladder filling accompanied by other symptoms such as increased daytime and nighttime frequency.” [20] “No proven urinary infection or other obvious pathology.” [20] This specification that the pain should be suprapubic and related to filling has been shown to result in decreasing the sensitivity by 34% [21]. Nevertheless, the European Association of Urology makes a strong case for integrating the medical, psychosocial, and sexual elements of care to engage the patient in a collaborative journey towards self-management [22].
Although firm data is lacking, the tendency in Europe seems to be to routinely evaluate the vast majority of patients with cystoscopy under anesthesia [23], [24], [25]. Various studies in Europe show the prevalence of Hunner lesions to be from 8% up to 55%, perhaps explaining the propensity for endoscopic evaluation [26], [27], [24].
Japan, Korea, Taiwan
The nomenclature and diagnosis of bladder pain syndrome is somewhat more complicated and opaque than the more distilled American and European concepts. The first attempts at harmonization were the result of the International Consultation on Interstitial Cystitis Japan 13 years ago [28]. A second meeting culminated with the development of Asian guidelines [29] and a follow-up meeting was devoted to the process of harmonization [30]. A fourth world-wide meeting is scheduled in 2018.
The current Asian thinking on what is referred to as bladder pain syndrome in the rest of the world was crystalized by Homma in a paper devoted to terminology [31]. The Japanese and Asian guidelines are basically identical [29], [32] and define interstitial cystitis as a disease of the urinary bladder diagnosed by three conditions: lower urinary tract symptoms, bladder pathology (such as Hunner lesion and mucosal bleeding after over distention) and exclusions of confusable diseases. There is no requirement for pain. The characteristic symptom complex is terms as hypersensitive bladder syndrome (HBS). HBS is defined as a bladder hypersensitivity, usually associated with urinary frequency, WITH OR WITHOUT bladder pain.
Thus, HBS would be a clinical entity that is more inclusive than pain syndromes. It incorporates patients complaining and not complaining of pain. HBS is a descriptive term that is appropriate for patients with symptoms of interstitial cystitis who do not fulfill the endoscopic findings of interstitial cystitis. Painful bladder syndrome (PBS) is HSB with pain. One can see the Asian thinking with regard to the relationships of these entities in figure 3. The general term “urgency frequency syndrome” also would include overactive bladder: urinary urgency, usually associated with urinary frequency, with or without urgency incontinence, the definition of the international continence society [17].
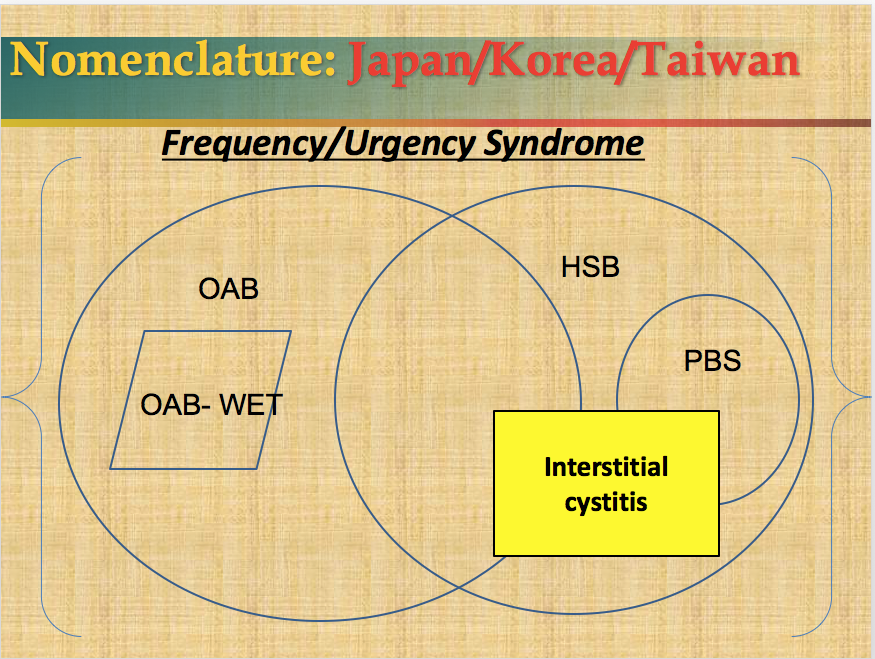
HSB = hypersensitive bladder syndrome
PBS = painful bladder syndrome
OAB = overactive bladder
Thus, in Asia the term bladder pain syndrome does not have a specific meaning. It is essential to do an endoscopic evaluation to diagnosis interstitial cystitis, but if the provider chooses not to do so, the diagnosis would either be HSB or PBS depending upon whether the patient had urinary symptoms with pain or without pain. One can see that it would be relatively easy to confuse overactive bladder with HSB in this schema and thus make pharmaceutical study reports somewhat problematic.
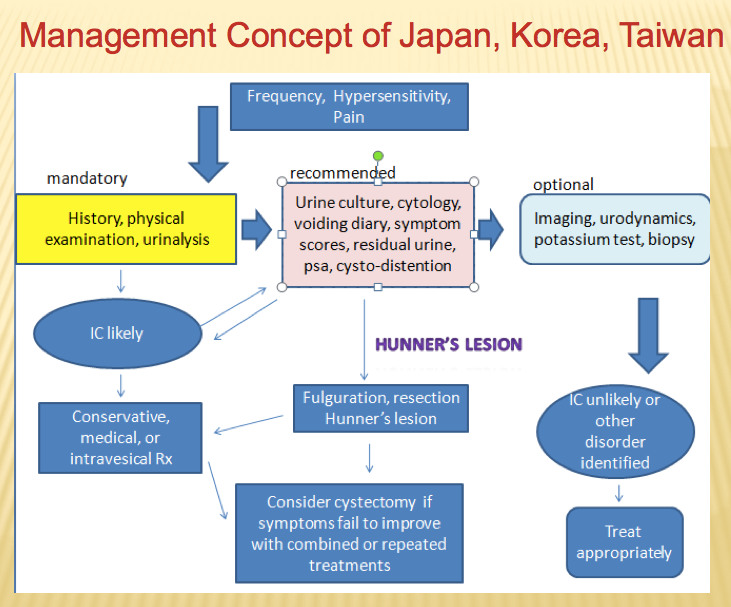
In Asia one can make a diagnosis of presumed interstitial cystitis on the basis of history, physical examination, and urinalysis alone and begin empiric therapy. In that sense, the American, European, and Asian concepts seem to merge. The Asian diagnostic/management algorithm is displayed in figure 4.
A recent survey on clinical practice of interstitial cystitis in Japan surveyed the number of IC patients, cystoscopic findings, diagnostic methods, and treatment modalities in 114 medical institutions [33]. The prevalence estimate was 3.56 per 100,000, very low but in line with other estimates when survey of providers was the methodology [34]. Of course this reflects patients requiring more intensive care overall. Ninety percent or more of patients underwent endoscopic evaluation and the overall prevalence of Hunner lesions was 29% and this finding was skewed depending upon the institution. Eighty-three percent of patients met the Asian definition of interstitial cystitis, 10% hypersensitive bladder syndrome, and 7% unknown. Evaluation included endoscopy, symptom and quality of life assessment, frequency-volume chart, urinalysis, urine cytology, urine culture, post void residual determination, uroflowmetry, and ultrasound.
In China, prevalence surveys have used the O’Leary Sant questionnaire as criteria [35]. Potassium sensitivity testing and hydrodistention are commonly employed [36]. Clinical history and urodynamics are also important parts of the diagnosis [37]. Complementary and alternative medicine, as an optional treatment, has been widely used [38]. In India retroperitoneal ultrasonography, measurement of post void residual, and cystoscopy with hydrodistention form the core for diagnosis [39].
International consultation
At this time there is no overwhelming international consensus on how to diagnose or manage bladder pain syndrome, and while Europe and North America agree on nomenclature, the Asian guideline differs. The International Consultation with members from Europe, North America, and Asia meets every 4 years to try to reach a consensus. Their diagnostic and treatment algorithm is presented in figure 5 [40]. The most significant harmonization to occur internationally is that all patients can be treated empirically on the basis of history, physical examination, urine culture, and elimination of likely confusable diseases without the need for invasive treatment at the onset of medical consultation.
References
[1] Berry SH, Elliott MN, Suttorp M, Bogart LM, Stoto MA, Eggers P, Nyberg L, Clemens JQ. Prevalence of symptoms of bladder pain syndrome/interstitial cystitis among adult females in the United States. J Urol. 2011 Aug;186(2):540-4. DOI: 10.1016/j.juro.2011.03.132[2] Suskind AM, Berry SH, Ewing BA, Elliott MN, Suttorp MJ, Clemens JQ. The prevalence and overlap of interstitial cystitis/bladder pain syndrome and chronic prostatitis/chronic pelvic pain syndrome in men: results of the RAND Interstitial Cystitis Epidemiology male study. J Urol. 2013 Jan;189(1):141-5. DOI: 10.1016/j.juro.2012.08.088
[3] Nordling J, Fall M, Hanno P. Global concepts of bladder pain syndrome (interstitial cystitis). World J Urol. 2012 Aug;30(4):457-64. DOI: 10.1007/s00345-011-0785-x
[4] Hanno PM, Burks DA, Clemens JQ, Dmochowski RR, Erickson D, Fitzgerald MP, Forrest JB, Gordon B, Gray M, Mayer RD, Newman D, Nyberg L Jr, Payne CK, Wesselmann U, Faraday MM; Interstitial Cystitis Guidelines Panel of the American Urological Association Education and Research, Inc. AUA guideline for the diagnosis and treatment of interstitial cystitis/bladder pain syndrome. J Urol. 2011 Jun;185(6):2162-70. DOI: 10.1016/j.juro.2011.03.064
[5] Waggoner J, Carline JD, Durning SJ. Is There a Consensus on Consensus Methodology? Descriptions and Recommendations for Future Consensus Research. Acad Med. 2016 May;91(5):663-8. DOI: 10.1097/ACM.0000000000001092
[6] Hanno P, Dmochowski R. Status of international consensus on interstitial cystitis/bladder pain syndrome/painful bladder syndrome: 2008 snapshot. Neurourol Urodyn. 2009;28(4):274-86. DOI: 10.1002/nau.20687
[7] Hanno PM, Landis JR, Matthews-Cook Y, Kusek J, Nyberg L Jr. The diagnosis of interstitial cystitis revisited: lessons learned from the National Institutes of Health Interstitial Cystitis Database study. J Urol. 1999 Feb;161(2):553-7.
[8] Diggs C, Meyer WA, Langenberg P, Greenberg P, Horne L, Warren JW. Assessing urgency in interstitial cystitis/painful bladder syndrome. Urology. 2007 Feb;69(2):210-4. DOI: 10.1016/j.urology.2006.09.053
[9] Hanno PM, Chapple CR, Cardozo LD. Bladder pain syndrome/interstitial cystitis: a sense of urgency. World J Urol. 2009 Dec;27(6):717-21. DOI: 10.1007/s00345-009-0439-4
[10] Parsons CL. Potassium sensitivity test. Tech Urol. 1996;2(3):171-3.
[11] Hanno P. Potassium sensitivity test for painful bladder syndrome/interstitial cystitis: con. J Urol. 2009 Aug;182(2):431-2, 434. DOI: 10.1016/j.juro.2009.05.070
[12] Hunner GL. A rare type of bladder ulcer in women; report of cases. Boston Med Surg Journal. 1915 May 6;172:660–4. DOI: 10.1056/NEJM191505061721802
[13] Wennevik GE, Meijlink JM, Hanno P, Nordling J. The Role of Glomerulations in Bladder Pain Syndrome: A Review. J Urol. 2016 Jan;195(1):19-25. DOI: 10.1016/j.juro.2015.06.112
[14] Hanno PM, Erickson D, Moldwin R, Faraday MM; American Urological Association. Diagnosis and treatment of interstitial cystitis/bladder pain syndrome: AUA guideline amendment. J Urol. 2015 May;193(5):1545-53. DOI: 10.1016/j.juro.2015.01.086
[15] Nordling J, Anjum FH, Bade JJ, Bouchelouche K, Bouchelouche P, Cervigni M, Elneil S, Fall M, Hald T, Hanus T, Hedlund H, Hohlbrugger G, Horn T, Larsen S, Leppilahti M, Mortensen S, Nagendra M, Oliveira PD, Osborne J, Riedl C, Sairanen J, Tinzl M, Wyndaele JJ. Primary evaluation of patients suspected of having interstitial cystitis (IC). Eur Urol. 2004 May;45(5):662-9. DOI: 10.1016/j.eururo.2003.11.021
[16] Ueda T. The legendary beginning of the International Consultation on Interstitial Cystitis. Int J Urol. 2003 Oct;10 Suppl:S1-2.
[17] Abrams P, Cardozo L, Fall M, Griffiths D, Rosier P, Ulmsten U, van Kerrebroeck P, Victor A, Wein A; Standardisation Sub-committee of the International Continence Society. The standardisation of terminology of lower urinary tract function: report from the Standardisation Sub-committee of the International Continence Society. Neurourol Urodyn. 2002;21(2):167-78.
[18] Baranowksi AP, Abrams P, Berger RE, Buffington CAT, de C. Williams AC, Hanno P, Loeser JD, Nickel CJ, Wesselmann U. Urogenital Pain – Time to Accept a New Approach to Phenotyping and, as a Consequence, Management. Eur Urol. 2008 Jan;53(1):33-6. DOI: 10.1016/j.eururo.2007.10.010
[19] van de Merwe JP, Nordling J, Bouchelouche P, Bouchelouche K, Cervigni M, Daha LK, Elneil S, Fall M, Hohlbrugger G, Irwin P, Mortensen S, van Ophoven A, Osborne JL, Peeker R, Richter B, Riedl C, Sairanen J, Tinzl M, Wyndaele JJ. Diagnostic criteria, classification, and nomenclature for painful bladder syndrome/interstitial cystitis: an ESSIC proposal. Eur Urol. 2008 Jan;53(1):60-7.
[20] Fall M, Baranowski AP, Elneil S, Engeler D, Hughes J, Messelink EJ, Oberpenning F, de C Williams AC; European Association of Urology. EAU guidelines on chronic pelvic pain. Eur Urol. 2010 Jan;57(1):35-48. DOI: 10.1016/j.eururo.2009.08.020
[21] Warren JW, Meyer WA, Greenberg P, Horne L, Diggs C, Tracy JK. Using the International Continence Society's definition of painful bladder syndrome. Urology. 2006 Jun;67(6):1138-42; discussion 1142-3. DOI: 10.1016/j.urology.2006.01.086
[22] Engeler DS, Baranowski AP, Dinis-Oliveira P, Elneil S, Hughes J, Messelink EJ, van Ophoven A, Williams AC; European Association of Urology. The 2013 EAU guidelines on chronic pelvic pain: is management of chronic pelvic pain a habit, a philosophy, or a science? 10 years of development. Eur Urol. 2013 Sep;64(3):431-9. DOI: 10.1016/j.eururo.2013.04.035
[23] Wyndaele JJ, Van Dyck J, Toussaint N. Cystoscopy and bladder biopsies in patients with bladder pain syndrome carried out following ESSIC guidelines. Scand J Urol Nephrol. 2009;43(6):471-5. DOI: 10.3109/00365590903199007
[24] Richter B, Hesse U, Hansen AB, Horn T, Mortensen SO, Nordling J. Bladder pain syndrome/interstitial cystitis in a Danish population: a study using the 2008 criteria of the European Society for the Study of Interstitial Cystitis. BJU Int. 2010 Mar;105(5):660-7. DOI: 10.1111/j.1464-410X.2009.08847.x
[25] Rourke W, Khan SA, Ahmed K, Masood S, Dasgupta P, Khan MS. Painful bladder syndrome/interstitial cystitis: aetiology, evaluation and management. Arch Ital Urol Androl. 2014 Jun 30;86(2):126-31. DOI: 10.4081/aiua.2014.2.126
[26] Rais-Bahrami S, Friedlander JI, Herati AS, Sadek MA, Ruzimovsky M, Moldwin RM. Symptom profile variability of interstitial cystitis/painful bladder syndrome by age. BJU Int. 2012 May;109(9):1356-9. DOI: 10.1111/j.1464-410X.2011.10481.x
[27] Logadottir Y, Fall M, Kåbjörn-Gustafsson C, Peeker R. Clinical characteristics differ considerably between phenotypes of bladder pain syndrome/interstitial cystitis. Scand J Urol Nephrol. 2012 Oct;46(5):365-70. DOI: 10.3109/00365599.2012.689008
[28] Ueda T, Sant GR, Hanno PM, Yoshimura N. Interstitial cystitis and frequency-urgency syndrome (OAB syndrome). Int J Urol. 2003 Oct;10 Suppl:S39-48.
[29] Homma Y, Ueda T, Tomoe H, Lin AT, Kuo HC, Lee MH, Lee JG, Kim DY, Lee KS; Interstitial cystitis guideline committee. Clinical guidelines for interstitial cystitis and hypersensitive bladder syndrome. Int J Urol. 2009 Jul;16(7):597-615. DOI: 10.1111/j.1442-2042.2009.02326.x
[30] Ueda T, Hanno P, Nordling J, Yoshimura N. The 3rd International Consultation on Interstitial Cystitis, Japan 2013. Int J Urol. 2014;21:1–2. DOI: 10.1111/iju.12306
[31] Homma Y. Lower urinary tract symptomatology: Its definition and confusion. Int J Urol. 2008 Jan;15(1):35-43. DOI: 10.1111/j.1442-2042.2007.01907.x
[32] Homma Y, Ueda T, Ito T, Takei M, Tomoe H. Japanese guideline for diagnosis and treatment of interstitial cystitis. Int J Urol. 2009 Jan;16(1):4-16. DOI: 10.1111/j.1442-2042.2008.02208.x
[33] Yamada Y, Nomiya A, Niimi A, Igawa Y, Ito T, Tomoe H, Takei M, Ueda T, Homma Y. A survey on clinical practice of interstitial cystitis in Japan. Transl Androl Urol. 2015 Oct;4(5):486-90. DOI: 10.3978/j.issn.2223-4683.2015.08.06
[34] Hanno P, Dinis P, Lin A, Nickel C, Nordling J, van Ophoven A, Ueda T. Bladder Pain Syndrome. In: Abrams P, Cardozo L, Khoury S, Wein A, editors. Incontinence. 5th ed. Paris: ICUD-EAU; 2013. p. 1583–649. Available from: http://www.icud.info/PDFs/INCONTINENCE%202013.pdf
[35] Li GZ, Zhang N, Du P, Yang Y, Wu SL, Xiao YX, Jin R, Liu L, Shen H, Dai Y. Risk factors for interstitial cystitis/painful bladder syndrome in patients with lower urinary tract symptoms: a Chinese multi-center study. Chin Med J (Engl). 2010 Oct;123(20):2842-6.
[36] Sun ZQ, Qian WQ, Xie DS, Song JD. [The study of diagnosis and treatment of interstitial cystitis]. Zhonghua Wai Ke Za Zhi. 2005 May;43(10):659-61.
[37] Flores-Carreras O, González-Ruiz MI, Martínez-Espinoza CJ, Monroy-Rodríguez F, Zaragoza-Torres RM. Interstitial cystitis/painful bladder syndrome: diagnostic evaluation and therapeutic response in a private urogynecology unit. Transl Androl Urol. 2015 Dec;4(6):620-3. DOI: 10.3978/j.issn.2223-4683.2015.10.11
[38] Pang R, Ali A. The Chinese approach to complementary and alternative medicine treatment for interstitial cystitis/bladder pain syndrome. Transl Androl Urol. 2015 Dec;4(6):653-61. DOI: 10.3978/j.issn.2223-4683.2015.08.10
[39] Mishra NN. Clinical presentation and treatment of bladder pain syndrome/interstitial cystitis (BPS/IC) in India. Transl Androl Urol. 2015 Oct;4(5):512-23. DOI: 10.3978/j.issn.2223-4683.2015.10.05
[40] Hanno PM, Cervigni M, Dinis P, Lin A, Nickel JC, Nordling J, van Ophoven A, Ueda T. Bladder pain syndrome. In: Abrams P, Cardoza L, Wagg A, Wein A, editors. Incontience. 6th ed. Paris: ICUD-EAU; 2017. p. 2203-2302.

