Treatment of chronic prostatitis/chronic pelvic pain syndrome – UPOINT
Dominic Tran-Nguyen 2
Daniel Shoskes 3
1 Des Moines University Medical College of Ostheopathic Medicine, Des Moines, Vereinigte Staaten
2 Des Moines University, Des Moines, Vereinigte Staaten
3 Glickman Urological and Kidney Institute, Cleveland Clinic, Cleveland, Vereinigte Staaten
Abstract
Chronic prostatitis/chronic pelvic pain syndrome (CP/CPPS) is a common condition, however many common therapies used in practice fail to show benefit when subjected to large randomized controlled trials. This discrepancy may be because CP/CPPS is a heterogeneous syndrome rather than one specific disease, which can explain the prior failure of any one therapy for all patients. In order to direct appropriate therapy, a six-point clinical phenotyping system was developed to evaluate patients with CP/CPPS. The clinical domains included are urinary symptoms, psychosocial dysfunction, organ-specific findings, infection, neurological/systemic complaints, and tenderness of muscles, producing the acronym UPOINT. Patients are diagnosed clinically for each domain and are given appropriate multimodal therapy for each positive domain. This approach is simple in theory and practice, and has proven effective in our hands for patients even after many years of failed therapies.
Summary of recommendations
- UPOINT is an approach to CP/CPPS that uses multimodal therapy based on the patient’s clinical phenotype. While untested in controlled randomized trials, published outcomes using individual therapies of varying evidence (see below) consistently show high levels of patient improvement (Level of Evidence 2b: Grade of Recommendation B).
- Anti-inflammatories should not be used as a monotherapy for the treatment of CP/CPPS, but should be considered as a component in multimodal therapy (Level of Evidence 1b: Grade of Recommendation A).
- Antibiotics: the clinical evidence suggests that antibacterial therapy should not be used as a monotherapy, particularly in patients who have failed antibacterial therapy previously (Level of Evidence 1a: Grade of Recommendation A). Antimicrobial therapy may, however, be considered for antimicrobial naïve patients (Level of Evidence 1b: Grade of Recommendation C).
- Alpha blocker therapy: We recommend alpha blocker therapy for the newly diagnosed, alpha blocker naïve patients with significant voiding symptoms (Level of Evidence 1a: Grade of Recommendation C). In patients previously treated with alpha blocker therapy, alpha blocker monotherapy is not recommended (Level of Evidence 1b: Grade of Recommendation A).
- Phytotherapy: Because of the few side effects of phytotherapy and the clinical efficacy of Quercetin and Cernilton suggested by these studies, these phytotherapies are recommended as a treatment modality of CP/CPPS (Cernilton Level of Evidence 1: Grade of Recommendation B) (Quercetin, Level of Evidence 1b: Grade of Recommendation A).
- Neuromodulatory therapy: Though there is some benefit in select patients using oral neuromodulatory therapy, the evidence does not support neuromodulatories as a monotherapy (Level of Evidence 1b: Grade of Recommendation B).
- 5 alpha reductase inhibitor therapies are not recommended for empiric monotherapy in male CP/CPPS patients (Level of Evidence 2: Grade of recommendation B). They should, however, be considered in patients with benign prostatic hyperplasia (BPH) (Level of Evidence 1a: Grade of recommendation A).
- Physical therapy: From clinical experience and uncontrolled clinical trials, it is believed that physical therapy may be beneficial in patients with pelvic floor muscle spasm and pain (Level of evidence 3: Grade of recommendation B).
Introduction
Chronic prostatitis/chronic pelvic pain syndrome (CP/CPPS) is a common condition that can cause a significant reduction in quality of life and substantial financial burden [1]. Symptoms include pelvic/genital pain, urinary frequency, and often erectile dysfunction which is not attributed to an other identifiable organ cause. Multiple factors may play a role in the pathophysiology of CPPS including initial urinary tract infection [2], intra-prostatic urinary reflux [3], inflammation, pelvic floor muscle spasm [4], or psychological traits like depression or stress [5]. However, none of these factors has been determined as the sole cause in majority of cases. Instead, a combination of these factors is likely contributing to CPPS and therefore therapy must likely be directed towards individual patient’s clinical phenotype. This is likely the reason why large studies of monotherapies for CPPS typically fail to show efficacy over placebo.
Because CP/CPPS is a syndrome with many presentations and not a specific disease, there is a need for an algorithm for phenotyping patients in order to direct appropriate treatment. This chapter will discuss monotherapies traditionally used for CP/CPPS, why these frequently tend to fail in a significant proportion of patients, the practical application of the UPOINT phenotyping system, and results of CP/CPPS treatment using UPOINT.
Methods
For this review, papers published in the English, peer-reviewed literature were evaluated. Papers published in non-peer-reviewed supplements were not included. The Medline database was used to identifying relevant studies published in the English literature over the last 20 years. Search terms included chronic prostatitis, chronic pelvic pain, as well as the multiple specific monotherapies (e.g., alpha blocker, antibiotic, anti-inflammatory, etc.). Only studies that defined a population of CP/CPPS men, were randomized placebo- or sham-controlled design, and employed a valid outcome measure were evaluated.
Monotherapies
Anti-inflammatories
Clinical trials regarding the use of anti-inflammatories as a monotherapy in patients with CP/CPPS have included rofecoxib [6], celecoxib [7], pentosan polysulfate [8], zafilukast [9], prednisone [10], and tanezumab [11]. These clinical trials yielded mixed results.
Rofecoxib and celecoxib have showed modest benefit, particularly when used at high dosages. Pentosan polysulfate, though showing symptom improvement, did not result in a significant change in CPSI score as compared to placebo. Tanezumab, a humanized monoclonal antibody that targets nerve growth factor, did not show any benefit in a non-selected population of CP/CPPS men. The use of zafirlukast and coriticosteroids had failed to improve CPSI scores as well. The clinical evidence suggests that anti-inflammatory as a monotherapy is not effective and should not be used in this manner.
Antibiotics
Antibiotics are widely prescribed and are, for many physicians, considered the first line therapy for patients with CP/CPPS. Despite its widespread use, there are only three small randomized controlled trials recorded in the literature [12], [ 13], [14]. These trials investigated the use of ciprofloxacin, levofloxacin, and tetracycline. One study investigating a four-week trial of tetracycline as compared to placebo showed significant benefit for CP/CPPS patients; however its authors judged quality of the study to be poor. Trials investigating the use of levofloxacin and ciprofloxacin showed significant benefit, but were underpowered when trying to establish an antibiotic effect as compared to placebo. The 12-week trial of tetracycline vs placebo yielded significant benefit, however, its results were marred by quality issues – including small numbers, selected patients, and anti-nanobacterial therapy which included tetracycline.
Clinical evidence does not support the empiric use of antibiotics in culture negative CPPS patients. However, there are reports that suggest symptomatic relief with antibiotic therapy, regardless of the presence of cultured uropathogenic bacteria [ 15], [16]. Meta-analysis of antimicrobial trials, including trials that did not use CPSI measurements as an outcome, did show small, but statistically significant benefit [17], [18]. However, whether or not these results translate into clinical significance has yet to be determined. A possible explanation of the benefit of antibiotics in culture negative CP/CPPS patients may be that in these cases, the patients may be infected with unculturable pathogens. Alternatively, some antibiotics have anti-inflammatory properties independent of their anti-bacterial characteristics [19], [20]. The clinical evidence suggests that antibacterial therapy should not be used as a monotherapy, particularly in patients who have failed antibacterial therapy previously. Antimicrobial therapy may, however, be considered for antimicrobial naïve patients.
Alpha blockers (Level of Evidence 1: Grade of Recommendation C)
Eight randomized placebo-controlled trials have evaluated the use of different alpha-adrenergic antagonists in CP/CPPS patients. Terazosin [21], tamsulosin [22], [23], alfuzosin [24], doxazosin [25], and silodosin [26] have shown benefit in CP/CPPS patients. Tamsulosin and alfuzosin [18] however have failed to show significant benefit in two large NIH-sponsored studies.
Many of the smaller alpha blocker studies do show benefit in selected CP/CPPS patients. A possible explanation for the failure of tamsulosin [14] and alfuzosin [27] in the two large NIH-sponsored studies would be the enlistment of patients who may have failed prior alpha-blocker therapy and those that did not have voiding symptoms. Meta-analyses [17], [18], [28] investigating alpha blocker therapy do reveal efficacy. At present, though not yet proven, it is still believed that patients with CP/CPPS and bothersome or measurable voiding symptoms may have the most benefit using alpha blockers as part of an overall therapeutic strategy. We therefore recommend alpha blocker therapy for the newly diagnosed, alpha blocker naïve patients with significant voiding symptoms. In patients previously treated with alpha blocker therapy and in those without urinary symptoms, alpha blocker monotherapy is not recommended.
Phytotherapy
Only two studies regarding phytotherapy met the criteria for this review. The phytotherapies investigated were quercetin [29] (an antioxidant anti-inflammatory product) and cernilton [30] (a standardized pollen extract). Quercetin improved symptoms in CP/CPPS patients when compared to placebo. Pollen extract showed efficacy in the reduction of pain and improvement of quality of life after 1 month of use. The mechanism of pain reduction is not established but quercetin is an antioxidant, anti-inflammatory and beta endorphin levels increase in prostate fluid during therapy. Because of the few side effects of phytotherapy and the clinical efficacy of quercetin and cernilton suggested by these studies, these phytotherapies are recommended as a treatment modality of CP/CPPS.
Neuromodulator therapy
Pregabalin was the only oral neuromodulatory randomized placebo-controlled study investigated in the treatment of CP/CPPS. One NIH sponsored study [31] comparing placebo to pregabalin showed a 6-point decrease in NIH-CPSI score, though these results were not statistically significant for the primary endpoint chosen. Pain scores and total CPSI, however, were significantly improved as compared to control. Though there is some benefit in select patients using oral neuromodulatory therapy, the evidence does not support neuromodulatories as a monotherapy (Level of Evidence 2: Grade of Recommendation B).
5 alpha reductase inhibitors and other hormone therapy
There is one randomized placebo-controlled trial comparing finasteride to placebo using CPSI score as a measurable outcome [32]. Another smaller study investigated mepartricin, an estrogen reducing agent [33].
Finasteride showed improvement in CPSI scores in CP/CPPS patients, though the results were not statistically significant. In the small study involving mepartricin, statistically significant improvement in CPSI scores were obtained when compared to placebo. Dutasteride was investigated as part of a long term, pre-planned analysis of older patients with CP/CPPS symptoms in a prostate cancer reduction trial and showed clinical benefit and a reduction in CPSI score over the long term [34]. Hormonal therapies, however, are not recommended for empiric monotherapy in male CP/CPPS patients. They should, however, be considered in patients with benign prostatic hyperplasia (BPH).
Physical therapies
Pain from CP/CPPS is often related to spasm of the pelvic floor muscles. Traditional western massage was compared with myofascial release physical therapy in men and women with chronic pelvic pain in a multicenter randomized NIH-sponsored study [35]. Other studies included extracorporeal shock wave treatment versus sham [36], percutaneous tibial nerve stimulation versus sham [37], electromagnetic therapy versus sham [38] and standard acupuncture [39] or electro acupuncture [40] versus sham treatment.
For the directed pelvic therapy versus traditional western massage, there was an improvement in CPSI scores in men, though not statistically significant. Randomized sham-controlled trials showed benefit with ESWT, acupuncture, percutaneous tibial nerve stimulation, and electro acupuncture.
From clinical experience and uncontrolled clinical trials, it is believed that physical therapy may be beneficial in patients with pelvic floor muscle spasm and pain.
Clinical phenotyping with UPOINT
The monotherapies discussed above have had limited success and one hypothesis would be that monotherapy fails due to the heterogeneous nature of CP/CPPS which is a syndrome rather than a single defined disorder. It would be ideal to clinically phenotype patients and target therapy to that phenotype. One such phenotyping system is UPOINT, named after the individual domains. The clinical domains are Urinary symptoms, Psychosocial dysfunction, Organ specific findings, Infection, Neurologic/Systemic, and Tenderness of muscles, which produces the acronym UPOINT. Each patient is evaluated clinically for involvement of each domain and symptom severity is assessed using the NIH-CPSI. This is followed by a multimodal therapeutic approach towards positive domains [41] (Figure 1). In studies on the validity of UPOINT, an increase in the number of positive UPOINT domains was found to correlate with increased total NIH-CPSI score, and the number of positive domains correlated with a longer duration of CP/CPPS symptoms [42], [43]. The greatest contribution to symptom severity was seen with the urinary, psychosocial, and tenderness domains [44]. These findings suggest that the UPOINT phenotyping system could prove useful as a clinical framework for directing multimodal therapy for treating CPPS.
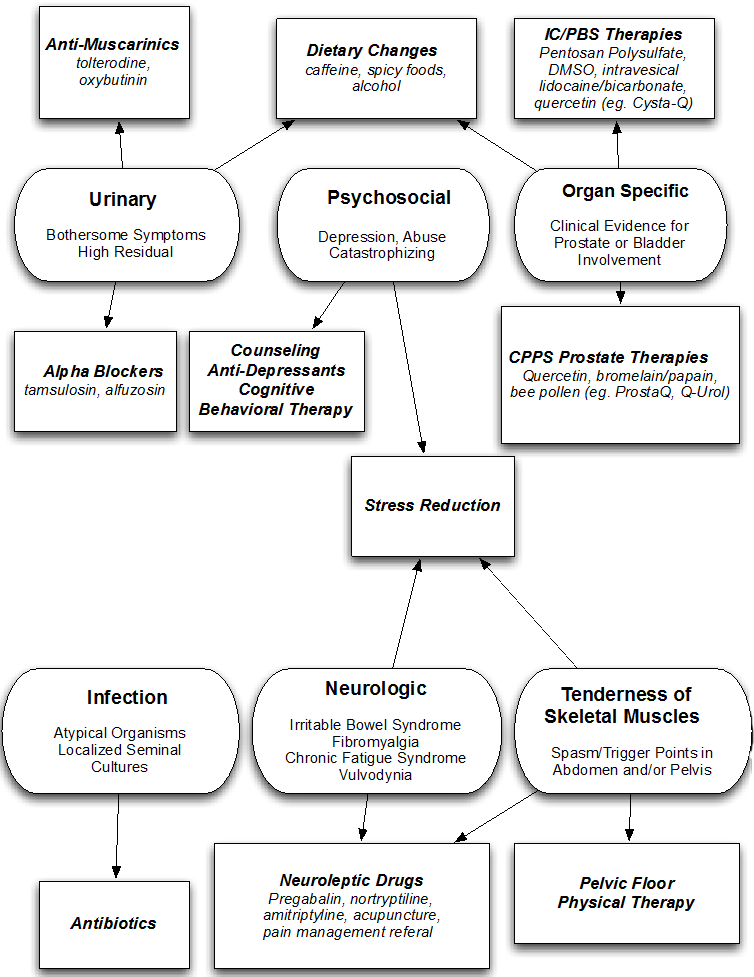
Figure 1: UPOINT domains and associated therapies
One prospective study evaluated the use of the multimodal therapy based on UPOINT phenotyping in 100 patients and compared response after at least 6 months [45]. 84% of patients had at least a 6-point decrease in CPSI, with an average drop of 12 points. All patients experienced significantly improved CPSI sub-scores from baseline. These results are significantly better than any prior large trials treating CPPS using monotherapy, suggesting the additional benefit of the UPOINT phenotyping system for directing therapy.
Practical guide to phenotyping with UPOINT
After evaluating a patient using UPOINT, a physician can use the positive phenotypes in order to guide the most suitable therapy. Patients are positive for the urinary domain if they bothersome urinary symptoms (e.g. increased/decreased frequency, weak stream, irritation, or obstruction), a CPSI urinary score greater than 4, or a high postvoid residual (PVR>100cc’s). Pain is the most frequent presenting symptom in patients, but many of these other urinary symptoms can be commonly found. Patients are positive for the psychosocial dysfunction domain of UPOINT with a demonstration of clinical depression, catastrophizing (feelings of helplessness and hopelessness about their condition), anxiety, stress and/or a history of sexual or other physical abuse on specific history or questionnaires. Patients positive for this domain are those with specific bladder or prostate symptoms. Organ specific findings include pain localized to the prostate on physical examination, hematospermia, or WBCs/markers of inflammation found in prostatic secretions, while bladder symptoms include pain relieved by bladder recycling (filling and voiding), ongoing inflammation, or a positive analgesic bladder challenge (relief of pain after infusion of the bladder with a topical anesthetic, i.e. lidocaine). Patients are positive for infection if there is a history or current presence of identifiable bacteria in prostatic fluid or evidence of chronic bacterial prostatitis. Neurologic or systemic symptoms can include pain outside of the lower abdomen/pelvis, fibromyalgia, chronic fatigue syndrome, irritable bowel syndrome, or diagnosis of another systemic or neurological disease. Finally, symptoms for muscle tenderness include muscle spasm and muscle or fascial ‘trigger points’ (palpable nodules in muscle that are tender to palpation).
Treatment guided by UPOINT
Urinary symptoms can be treated with alpha-blockers or anticholinergic medications. Psychosocial symptoms, or “catastrophizing”, are treated with psychological counseling and stress reduction. Organ specific symptoms related to the prostate are treated with bioflavonoids such as quercetin. Bladder symptoms indicative of interstitial cystitis can include Infections are treated with adequate courses of culture-directed therapies. Neurologic or systemic symptoms are treated with tricyclic antidepressants or gabapentin/neuroleptics. Lastly, muscle tenderness is treated with a pelvic floor physical therapy and/or trigger point injections. For example, a patient with urinary and organ specific domains could be treated with an alpha-blocker and quercetin, while another with neurologic and tenderness would be treated with pregabalin and pelvic floor physical therapy.
An online resource has been made available for use by urologists, where one enters patient data and is given the UPOINT clinical phenotype with suggested therapies. A web-based algorithm is available at http://www.upointmd.com.
Subsequent studies on UPOINT
While UPOINT was developed in order to comprise the significant symptoms of CPPS, there is potential for the addition of other domains if these domains added to the diagnostic value of the system. One European study investigated whether the addition of another domain (sexual dysfunction) could improve the correlation between UPOINT positive domains and CPSI scores in two separate populations. The traditional UPOINT system correlated with symptom severity in the Italian, but not in the German group . The investigated modified phenotyping system (UPOINTS), using an additional sexual dysfunction domain, correlated significantly with NIH-CPSI scores in the German cohort [46]. Another Canadian study found the addition of this sexual dysfunction domain improved the system’s correlation with quality of life [47]. This finding was further studied in a population of one hundred patients in the US [48]. While 28% of men with CP/CPPS reported bothersome erectile dysfunction, addition of the sexual dysfunction domain decreased the correlation between the UPOINT system and symptom severity. Additionally, NIH-CPSI scores, pain sub-scores, and quality of life measures were unaffected by erectile dysfunction. Therefore, inclusion of a sexual domain did not appear to add value in this patient population.
Conclusions
While there have been advances in the research for the treatment of men with CP/CPPS over the last 15 years, a solely evidence-based approach to treatment yields insufficient results for most patients. No one individual treatment that shows significant clinical efficacy to be recommended as a monotherapy for CP/CPPS. A multi-modal therapeutic approach to treatment specifically directed to each individual patients’ clinical phenotypic profile is likely the best management strategy. Use of the UPOINT phenotyping system allows for this individualization and potentially better outcomes, despite the current lack of randomized controlled trials evidencing this.
Conflict of interest
Daniel Shoskes: Farr Laboratories, Triurol
References
[1] Shoskes DA. Chronic prostatitis/chronic pelvic pain syndrome. Totowa: Humana Press; 2008.[2] Persson BE, Ronquist G. Evidence for a mechanistic association between nonbacterial prostatitis and levels of urate and creatinine in expressed prostatic secretion. J Urol. 1996 Mar;155(3):958-60. DOI: 10.1016/S0022-5347(01)66357-2
[3] He L, Wang Y, Long Z, Jiang C. Clinical significance of IL-2, IL-10, and TNF-alpha in prostatic secretion of patients with chronic prostatitis. Urology. 2010 Mar;75(3):654-7. DOI: 10.1016/j.urology.2009.09.061
[4] Westesson KE, Shoskes DA. Chronic prostatitis/chronic pelvic pain syndrome and pelvic floor spasm: can we diagnose and treat? Curr Urol Rep. 2010 Jul;11(4):261-4. DOI: 10.1007/s11934-010-0111-y
[5] Tripp DA, Nickel JC, Wang Y, Litwin MS, McNaughton-Collins M, Landis JR, Alexander RB, Schaeffer AJ, O'Leary MP, Pontari MA, Fowler JE Jr, Nyberg LM, Kusek JW; National Institutes of Health-Chronic Prostatitis Collaborative Research Network (NIH-CPCRN) Study Group. Catastrophizing and pain-contingent rest predict patient adjustment in men with chronic prostatitis/chronic pelvic pain syndrome. J Pain. 2006 Oct;7(10):697-708. DOI: 10.1016/j.jpain.2006.03.006
[6] Nickel JC, Pontari M, Moon T, Gittelman M, Malek G, Farrington J, Pearson J, Krupa D, Bach M, Drisko J; Rofecoxib Prostatitis Investigator Team. A randomized, placebo controlled, multicenter study to evaluate the safety and efficacy of rofecoxib in the treatment of chronic nonbacterial prostatitis. J Urol. 2003 Apr;169(4):1401-5. DOI: 10.1097/01.ju.0000054983.45096.16
[7] Zhao WP, Zhang ZG, Li XD, Yu D, Rui XF, Li GH, Ding GQ. Celecoxib reduces symptoms in men with difficult chronic pelvic pain syndrome (Category IIIA). Braz J Med Biol Res. 2009 Oct;42(10):963-7. DOI: 10.1590/S0100-879X2009005000021
[8] Nickel JC, Forrest JB, Tomera K, Hernandez-Graulau J, Moon TD, Schaeffer AJ, Krieger JN, Zeitlin SI, Evans RJ, Lama DJ, Neal DE Jr, Sant GR. Pentosan polysulfate sodium therapy for men with chronic pelvic pain syndrome: a multicenter, randomized, placebo controlled study. J Urol. 2005 Apr;173(4):1252-5. DOI: 10.1097/01.ju.0000159198.83103.01
[9] Goldmeier D, Madden P, McKenna M, Tamm N. Treatment of category III A prostatitis with zafirlukast: a randomized controlled feasibility study. Int J STD AIDS. 2005 Mar;16(3):196-200. DOI: 10.1258/0956462053420239
[10] Bates SM, Hill VA, Anderson JB, Chapple CR, Spence R, Ryan C, Talbot MD. A prospective, randomized, double-blind trial to evaluate the role of a short reducing course of oral corticosteroid therapy in the treatment of chronic prostatitis/chronic pelvic pain syndrome. BJU Int. 2007 Feb;99(2):355-9. DOI: 10.1111/j.1464-410X.2007.06667.x
[11] Nickel JC, Atkinson G, Krieger JN, Mills IW, Pontari M, Shoskes DA, Crook TJ. Preliminary assessment of safety and efficacy in proof-of-concept, randomized clinical trial of tanezumab for chronic prostatitis/chronic pelvic pain syndrome. Urology. 2012 Nov;80(5):1105-10. DOI: 10.1016/j.urology.2012.07.035
[12] Zhou Z, Hong L, Shen X, Rao X, Jin X, Lu G, Li L, Xiong E, Li W, Zhang J, Chen Z, Pan J, Song B. Detection of nanobacteria infection in type III prostatitis. Urology. 2008 Jun;71(6):1091-5. DOI: 10.1016/j.urology.2008.02.041
[13] Nickel JC, Downey J, Clark J, Casey RW, Pommerville PJ, Barkin J, Steinhoff G, Brock G, Patrick AB, Flax S, Goldfarb B, Palmer BW, Zadra J. Levofloxacin for chronic prostatitis/chronic pelvic pain syndrome in men: a randomized placebo-controlled multicenter trial. Urology. 2003 Oct;62(4):614-7. DOI: 10.1016/S0090-4295(03)00583-1
[14] Alexander RB, Propert KJ, Schaeffer AJ, Landis JR, Nickel JC, O'Leary MP, Pontari MA, McNaughton-Collins M, Shoskes DA, Comiter CV, Datta NS, Fowler JE Jr, Nadler RB, Zeitlin SI, Knauss JS, Wang Y, Kusek JW, Nyberg LM Jr, Litwin MS; Chronic Prostatitis Collaborative Research Network. Ciprofloxacin or tamsulosin in men with chronic prostatitis/chronic pelvic pain syndrome: a randomized, double-blind trial. Ann Intern Med. 2004 Oct;141(8):581-9. DOI: 10.7326/0003-4819-141-8-200410190-00005
[15] Nickel JC, Downey J, Johnston B, Clark J; Canadian Prostatitis Research Group. Predictors of patient response to antibiotic therapy for the chronic prostatitis/chronic pelvic pain syndrome: a prospective multicenter clinical trial. J Urol. 2001 May;165(5):1539-44. DOI: 10.1016/S0022-5347(05)66344-6
[16] Nickel JC, Xiang J. Clinical significance of nontraditional bacterial uropathogens in the management of chronic prostatitis. J Urol. 2008 Apr;179(4):1391-5. DOI: 10.1016/j.juro.2007.11.081.
[17] Anothaisintawee T, Attia J, Nickel JC, Thammakraisorn S, Numthavaj P, McEvoy M, Thakkinstian A. Management of chronic prostatitis/chronic pelvic pain syndrome: a systematic review and network meta-analysis. JAMA. 2011 Jan 5;305(1):78-86. DOI: 10.1001/jama.2010.1913
[18] Thakkinstian A, Attia J, Anothaisintawee T, Nickel JC. α-blockers, antibiotics and anti-inflammatories have a role in the management of chronic prostatitis/chronic pelvic pain syndrome. BJU Int. 2012 Oct;110(7):1014-22. DOI: 10.1111/j.1464-410X.2012.11088.x
[19] Ogino H, Fujii M, Ono M, Maezawa K, Hori S, Kizu J. In vivo and in vitro effects of fluoroquinolones on lipopolysaccharide-induced pro-inflammatory cytokine production. J Infect Chemother. 2009 Jun;15(3):168-73. DOI: 10.1007/s10156-009-0680-1
[20] Tsivkovskii R, Sabet M, Tarazi Z, Griffith DC, Lomovskaya O, Dudley MN. Levofloxacin reduces inflammatory cytokine levels in human bronchial epithelia cells: implications for aerosol MP-376 (levofloxacin solution for inhalation) treatment of chronic pulmonary infections. FEMS Immunol Med Microbiol. 2011 Mar;61(2):141-6. DOI: 10.1111/j.1574-695X.2010.00755.x
[21] Cheah PY, Liong ML, Yuen KH, Teh CL, Khor T, Yang JR, Yap HW, Krieger JN. Terazosin therapy for chronic prostatitis/chronic pelvic pain syndrome: a randomized, placebo controlled trial. J Urol. 2003 Feb;169(2):592-6. DOI: 10.1097/01.ju.0000042927.45683.6c
[22] Chen Y, Wu X, Liu J, Tang W, Zhao T, Zhang J. Effects of a 6-month course of tamsulosin for chronic prostatitis/chronic pelvic pain syndrome: a multicenter, randomized trial. World J Urol. 2011 Jun;29(3):381-5. DOI: 10.1007/s00345-010-0537-3
[23] Nickel JC, Narayan P, McKay J, Doyle C. Treatment of chronic prostatitis/chronic pelvic pain syndrome with tamsulosin: a randomized double blind trial. J Urol. 2004 Apr;171(4):1594-7. DOI: 10.1097/01.ju.0000117811.40279.19
[24] Mehik A, Alas P, Nickel JC, Sarpola A, Helström PJ. Alfuzosin treatment for chronic prostatitis/chronic pelvic pain syndrome: a prospective, randomized, double-blind, placebo-controlled, pilot study. Urology. 2003 Sep;62(3):425-9. DOI: 10.1016/S0090-4295(03)00466-7
[25] Tuğcu V, Taşçi AI, Fazlioğlu A, Gürbüz G, Ozbek E, Sahin S, Kurtuluş F, Cek M. A placebo-controlled comparison of the efficiency of triple- and monotherapy in category III B chronic pelvic pain syndrome (CPPS). Eur Urol. 2007 Apr;51(4):1113-7; discussion 1118. DOI: 10.1016/j.eururo.2006.09.036
[26] Nickel JC, O'Leary MP, Lepor H, Caramelli KE, Thomas H, Hill LA, Hoel GE. Silodosin for men with chronic prostatitis/chronic pelvic pain syndrome: results of a phase II multicenter, double-blind, placebo controlled study. J Urol. 2011 Jul;186(1):125-31. DOI: 10.1016/j.juro.2011.03.028
[27] Nickel JC, Krieger JN, McNaughton-Collins M, Anderson RU, Pontari M, Shoskes DA, Litwin MS, Alexander RB, White PC, Berger R, Nadler R, O'Leary M, Liong ML, Zeitlin S, Chuai S, Landis JR, Kusek JW, Nyberg LM, Schaeffer AJ; Chronic Prostatitis Collaborative Research Network. Alfuzosin and symptoms of chronic prostatitis-chronic pelvic pain syndrome. N Engl J Med. 2008 Dec;359(25):2663-73. DOI: 10.1056/NEJMoa0803240
[28] Yang G, Wei Q, Li H, Yang Y, Zhang S, Dong Q. The effect of alpha-adrenergic antagonists in chronic prostatitis/chronic pelvic pain syndrome: a meta-analysis of randomized controlled trials. J Androl. 2006 Nov-Dec;27(6):847-52. DOI: 10.2164/jandrol.106.000661
[29] Shoskes DA, Zeitlin SI, Shahed A, Rajfer J. Quercetin in men with category III chronic prostatitis: a preliminary prospective, double-blind, placebo-controlled trial. Urology. 1999 Dec;54(6):960-3. DOI: 10.1016/S0090-4295(99)00358-1
[30] Wagenlehner FM, Schneider H, Ludwig M, Schnitker J, Brähler E, Weidner W. A pollen extract (Cernilton) in patients with inflammatory chronic prostatitis-chronic pelvic pain syndrome: a multicentre, randomised, prospective, double-blind, placebo-controlled phase 3 study. Eur Urol. 2009 Sep;56(3):544-51. DOI: 10.1016/j.eururo.2009.05.046
[31] Pontari MA, Krieger JN, Litwin MS, White PC, Anderson RU, McNaughton-Collins M, Nickel JC, Shoskes DA, Alexander RB, O'Leary M, Zeitlin S, Chuai S, Landis JR, Cen L, Propert KJ, Kusek JW, Nyberg LM Jr, Schaeffer AJ; Chronic Prostatitis Collaborative Research Network-2. Pregabalin for the treatment of men with chronic prostatitis/chronic pelvic pain syndrome: a randomized controlled trial. Arch Intern Med. 2010 Sep;170(17):1586-93. DOI: 10.1001/archinternmed.2010.319
[32] Nickel JC, Downey J, Pontari MA, Shoskes DA, Zeitlin SI. A randomized placebo-controlled multicentre study to evaluate the safety and efficacy of finasteride for male chronic pelvic pain syndrome (category IIIA chronic nonbacterial prostatitis). BJU Int. 2004 May;93(7):991-5. DOI: 10.1111/j.1464-410X.2003.04766.x
[33] De Rose AF, Gallo F, Giglio M, Carmignani G. Role of mepartricin in category III chronic nonbacterial prostatitis/chronic pelvic pain syndrome: a randomized prospective placebo-controlled trial. Urology. 2004 Jan;63(1):13-6. DOI: 10.1016/j.urology.2003.08.006
[34] Nickel JC, Roehrborn C, Montorsi F, Wilson TH, Rittmaster RS. Dutasteride reduces prostatitis symptoms compared with placebo in men enrolled in the REDUCE study. J Urol. 2011 Oct;186(4):1313-8. DOI: 10.1016/j.juro.2011.05.071
[35] FitzGerald MP, Anderson RU, Potts J, Payne CK, Peters KM, Clemens JQ, Kotarinos R, Fraser L, Cosby A, Fortman C, Neville C, Badillo S, Odabachian L, Sanfield A, O'Dougherty B, Halle-Podell R, Cen L, Chuai S, Landis JR, Mickelberg K, Barrell T, Kusek JW, Nyberg LM; Urological Pelvic Pain Collaborative Research Network. Randomized multicenter feasibility trial of myofascial physical therapy for the treatment of urological chronic pelvic pain syndromes. J Urol. 2009 Aug;182(2):570-80. DOI: 10.1016/j.juro.2009.04.022
[36] Zimmermann R, Cumpanas A, Miclea F, Janetschek G. Extracorporeal shock wave therapy for the treatment of chronic pelvic pain syndrome in males: a randomised, double-blind, placebo-controlled study. Eur Urol. 2009 Sep;56(3):418-24. DOI: 10.1016/j.eururo.2009.03.043
[37] Kabay S, Kabay SC, Yucel M, Ozden H. Efficiency of posterior tibial nerve stimulation in category IIIB chronic prostatitis/chronic pelvic pain: a Sham-Controlled Comparative Study. Urol Int. 2009;83(1):33-8. DOI: 10.1159/000224865
[38] Rowe E, Smith C, Laverick L, Elkabir J, Witherow RO, Patel A. A prospective, randomized, placebo controlled, double-blind study of pelvic electromagnetic therapy for the treatment of chronic pelvic pain syndrome with 1 year of followup. J Urol. 2005 Jun;173(6):2044-7. DOI: 10.1097/01.ju.0000158445.68149.38
[39] Lee SW, Liong ML, Yuen KH, Leong WS, Chee C, Cheah PY, Choong WP, Wu Y, Khan N, Choong WL, Yap HW, Krieger JN. Acupuncture versus sham acupuncture for chronic prostatitis/chronic pelvic pain. Am J Med. 2008 Jan;121(1):79.e1-7. DOI: 10.1016/j.amjmed.2007.07.033
[40] Lee SH, Lee BC. Electroacupuncture relieves pain in men with chronic prostatitis/chronic pelvic pain syndrome: three-arm randomized trial. Urology. 2009 May;73(5):1036-41. DOI: 10.1016/j.urology.2008.10.047
[41] Shoskes DA, Nickel JC, Rackley RR, Pontari MA. Clinical phenotyping in chronic prostatitis/chronic pelvic pain syndrome and interstitial cystitis: a management strategy for urologic chronic pelvic pain syndromes. Prostate Cancer Prostatic Dis. 2009;12(2):177-83. DOI: 10.1038/pcan.2008.42
[42] Shoskes DA, Nickel JC, Dolinga R, Prots D. Clinical phenotyping of patients with chronic prostatitis/chronic pelvic pain syndrome and correlation with symptom severity. Urology. 2009 Mar;73(3):538-42; discussion 542-3. DOI: 10.1016/j.urology.2008.09.074
[43] Hedelin HH. Evaluation of a modification of the UPOINT clinical phenotype system for the chronic pelvic pain syndrome. Scand J Urol Nephrol. 2009;43(5):373-6. DOI: 10.3109/00365590903164514
[44] Samplaski MK, Li J, Shoskes DA. Clustering of UPOINT domains and subdomains in men with chronic prostatitis/chronic pelvic pain syndrome and contribution to symptom severity. J Urol. 2012 Nov;188(5):1788-93. DOI: 10.1016/j.juro.2012.07.036
[45] Shoskes DA, Nickel JC, Kattan MW. Phenotypically directed multimodal therapy for chronic prostatitis/chronic pelvic pain syndrome: a prospective study using UPOINT. Urology. 2010 Jun;75(6):1249-53. DOI: 10.1016/j.urology.2010.01.021
[46] Magri V, Wagenlehner F, Perletti G, Schneider S, Marras E, Naber KG, Weidner W. Use of the UPOINT chronic prostatitis/chronic pelvic pain syndrome classification in European patient cohorts: sexual function domain improves correlations. J Urol. 2010 Dec;184(6):2339-45. DOI: 10.1016/j.juro.2010.08.025
[47] Davis SN, Binik YM, Amsel R, Carrier S. Is a sexual dysfunction domain important for quality of life in men with urological chronic pelvic pain syndrome? Signs "UPOINT" to yes. J Urol. 2013 Jan;189(1):146-51. DOI: 10.1016/j.juro.2012.08.083
[48] Samplaski MK, Li J, Shoskes DA. Inclusion of erectile domain to UPOINT phenotype does not improve correlation with symptom severity in men with chronic prostatitis/chronic pelvic pain syndrome. Urology. 2011 Sep;78(3):653-8. DOI: 10.1016/j.urology.2011.04.016

