Training of sound localization in adult cochlear implant users with single-sided deafness
Willem Alexander Klatt 1Kirsten Oberländer 2
Marius Markgraf 1
Stefan T. Kamin 3
Rainer Martin 1
Christiane Völter 2
1 Institute Communication Acoustics, Ruhr-University Bochum, Germany
2 St. Elisabeth-Hospital Bochum, Cochlear Implant Center, Ruhr-University Bochum, Germany
3 Human Centered Innovation Group, Fraunhofer Institute for Integrated Circuits, Erlangen, Germany
Abstract
In this paper, we present the results of a pilot study investigating the feasibility of a training of sound localization abilities in cochlear implant (CI) users with single-sided deafness (SSD). The training program has been implemented in a cohort of 20 adult postlingually deafened SSD CI users across a period of four weeks. The training setup consisted of 7 loudspeakers placed on the azimuth in steps of 30 degrees. The present data clearly showed an improvement in localization skills, mainly for acoustic sources placed in the frontal directions. Further studies are necessary to confirm the benefits of localization training in a larger sample including a control group, with the aim to establish localization training as a regular part in CI rehabilitation settings.
Keywords
cochlear implantation, single-sided deafness, training, localization, rehabilitation
1 Introduction
Binaural hearing relies on the brain’s ability to accurately compare timing and intensity differences between the two ears [4] and is an important skill in everyday life for orientation and speech comprehension in complex acoustic situations. Cochlear implantation (CI) is the treatment of choice in single-sided deafness (SSD) in adults as well as in children [1], [3], as it allows the restoration of bilateral input to the auditory system and possibly also binaural hearing.
Although CI improves sound localization in SSD CI users [5], [19], SSD CI users do not perform as well as normal-hearing individuals in directional hearing [6], [12], [21]. However, postoperative rehabilitation after cochlear implantation strongly focuses on the improvement in speech understanding. Localization training has rarely been included so far, but it might be an option to improve also these skills in SSD CI users.
Up to now, spatial training has been explored mostly in studies in hearing-impaired subjects [10], in unaided SSD [7] or in unilateral CI users [17]. To the best of our knowledge, there is only one study analyzing localization training in SSD CI users in a virtual acoustics setup with individualized head-related transfer functions, but neglecting natural head movements [16]. Therefore, the aim of the present study was to analyze the feasibility of a standardized and compact four-week training program using a simple physical loudspeaker setup.
2 Materials and methods
2.1 Participants
This study examined 20 adult SSD CI users (10 female, 10 male). The mean age at the time of the study was 53.8 years (SD: 13.3 years), and the duration of deafness averaged 120.8 months (SD: 178.4 months). Sudden hearing loss was the most frequently reported cause of deafness (in 65% of cases). No participant suffered from severe psychological, cognitive or physiological impairments. All but one participants used MED-EL implants (MED-EL GmbH, Innsbruck, Austria), with either FSP (two participants) or FS4 (17 participants) coding strategies, and one participant used a cochlear implant (Cochlear Ltd., Sydney, Australia) and the ACE coding strategy. The mean CI experience was 19.6 months (SD: 19.4 months).
2.2 Training procedure
All participants received a four-week localization training with sessions of about 30 minutes twice per week. Seven loudspeakers were arranged in a semicircle at the positions –90° (position to the left-hand side of the listener), –60°, –30°, 0°, 30°, 60°, and 90°, according to Van de Heyning et al. [18]. Five different real-world sounds were presented in a randomized order: a classic telephone ring, a doorbell, a car horn, and the German words “eins” and “da” (corresponding to “one” and “there”), spoken by a female voice. Stimuli were presented with a nominal duration of one second and delivered with a sound pressure level of 65 dB SPL ±3 dB. Subjects were instructed to keep their heads directed toward the 0° direction. In each training session, 50 stimuli were played. Feedback was given immediately after the listener’s answer and in case of an incorrect answer the stimulus was repeated. The first session of the eight training sessions implemented a simple lateralization training, using only the –90°, 0°, 90° and the –60°, 0°, 60° loudspeakers.
2.3 Testing procedure
Localization ability was assessed using the loudspeaker setup described in the consensus paper [18]. Two stimuli were generated by filtering one-second CCITT noise signals using the head-related transfer functions of the left and right ears of the KEMAR head-and-torso simulator [15]. The spectral shape was modified to limit the use of monaural HRTF cues and force the subjects to focus on interaural cues. These signals were presented at three different volumes (60, 65, and 70 dB SPL), resulting in six unique stimuli. These stimuli were played in random order through the seven loudspeakers of the same system used for training. This resulted in 42 stimuli for the test. The assessment was conducted before training (“pre”) and after training (“post”). A final (follow-up) test was performed 3 months after the completion of the training.
For the objective assessment of directional hearing, the root mean-squared error (RMSE) and the mean absolute error (MAE) between the true and predicted angles of sound incidence were used.
2.4 Statistical analysis
The Welch-variant of the t-test was used to analyze and assess whether there were statistically significant changes in the RMSE values at the various test time points. The same test procedure was also used to analyze the pre- and post-directional hearing tests with and without a CI, respectively. For the individual evaluation of the angular errors made in each directional hearing test, we used the nonparametric Wilcoxon signed-rank test [8], as the data were not normally distributed. The significance levels for all tests were *=p<0.05, **=p<0.01, and ***=p<0.001.
To examine the learning process, the data of the training sessions 2–8 were used to optimize generalized linear mixed models using the BOBYQA algorithm [2]. The aim was to verify the training effect and to identify influencing factors, thereby enabling the prediction of improvements in directional hearing based on the characteristics of SSD CI probands. In this analysis, the first training session was omitted because it implemented an easier task as only 3 loudspeakers were used.
3 Results
3.1 Improvement of directional hearing
Table 1 [Tab. 1] summarizes the mean, median, and SD of the RMSE and MAE of the 20 participants. As a result of the training sessions, both the RMSE and the MAE indicated an improvement in localization, and a comparable performance in the follow-up test.
Table 1: RMSE und MAE in degree of pre-tests, post-tests and follow-up testing (after 12 weeks) of the cohort of 20 SSD CI users
The RMSE per presented direction is shown for the pre-test and post-test in Figure 1 [Fig. 1]. Cochlear implant users benefitted most from the training on the implanted side. Significant improvements occurred at the frontal angles of 0° (p<0.05) and of 30° (p<0.01). This improvement was still measurable 12 weeks after the post-test without a significant deterioration (p=0.68).
Figure 1: RMSE for each presented direction, before training (Pre-test) and after training (Post-test). Directions were normalized such that negative angles correspond to the acoustic-hearing side for all participants. Means (green-dashed) and t-test significance levels: *=p<0.05; **=p<0.01; ***=p<0.001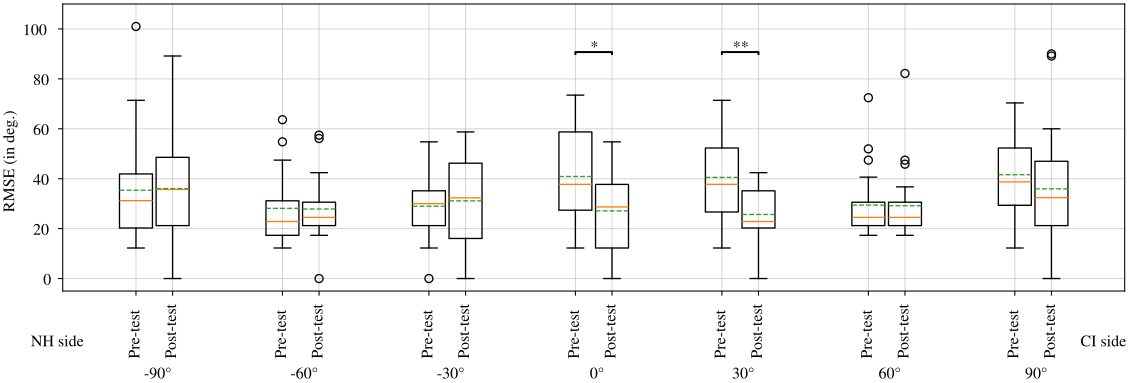
3.2 Analysis of learning progress
The longitudinal analysis of training sessions confirmed highly significant improvements (p<0.001) of the localization ability of the participants. The training sessions showed a linear improvement, with the training effect becoming apparent primarily for frontal stimuli (especially 0°; see Figure 2 [Fig. 2]), and slower learning curves for the other directions.
Figure 2: Direction-specific learning trajectories (sessions 2–8). Center direction (0°) shows robust learning, lateral positions show slower improvement.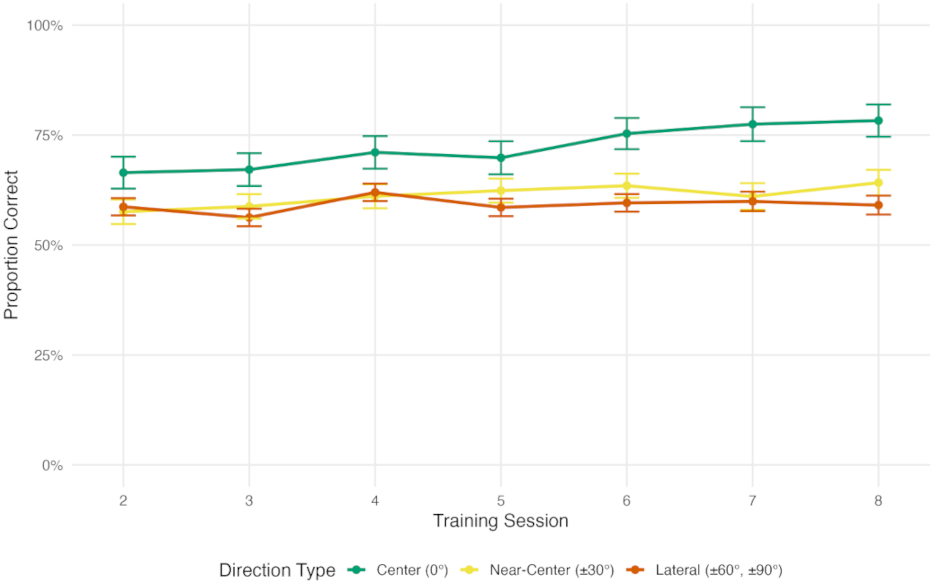
The reaction time also significantly declined (p=0.002) over the course of the training (see Figure 3 [Fig. 3]), and some subjects were able to localize the incident sounds correctly within 3 seconds in about 75% of the trials.
Figure 3: Relationship between reaction time and accuracy across Sessions 2–8. The figure shows reaction time improvements over training.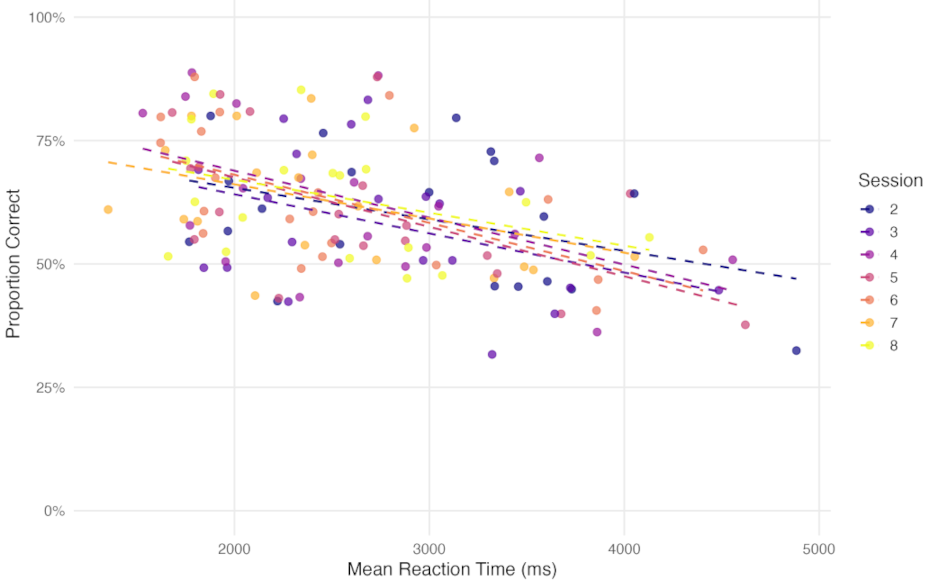
Probands who performed better in the pre-test also performed significantly better during the training and at the end of the training (p=0.011). Older participants performed significantly worse during the training than younger patients but age did not affect learning rate (p<0.001). A longer duration of deafness led to significantly worse performance (p=0.03). It is also noteworthy to mention that strong tinnitus (in 3 out of the 20 participants) had a negative impact on localization ability only at the beginning of training.
4 Discussion
In this work, we presented a pilot study for training spatial localization in adult SSD CI users. Hereby, we employed the training setup and method developed in [11], [18], and extended our previous study to a larger number of participants.
To make the training more relevant and thus more acceptable to the participants we used real-world sounds and a physical loudspeaker setup during the training sessions. All participants completed the training program without gaps. On average, the training resulted in an improvement, especially in the frontal direction. Thus, the training benefits go hand-in-hand with the improved sound localization on the side of the CI in SSD users, e.g., [20]. Furthermore, the improvements in directional hearing remained significant even 12 weeks after the post-test.
The use of filtered noise signals for testing shows that the participants’ improved localization ability is not linked to the type of stimulus. This observation opens the door for the introduction of more ecological and thus more motivating training setups that could be explored in future works. However, the use of real-world stimuli also limits a direct comparison with other localization studies which used different speaker setups and stimuli, as summarized, e.g., in [11].
Unlike in [14], we were able to show that even patients who had a low pre-test localization performance or a low training success improved to the extent that they did no longer localize exclusively on the normal-hearing side in the post-test.
Age and duration of deafness had a negative impact on directional hearing in younger participants and participants with a shorter duration of deafness demonstrated significantly better localization abilities during all stages of the training. Older participants, however, learned at similar rates.
Furthermore, even in SSD patients with pronounced tinnitus, a training effect was detected and directional hearing ability improved sufficiently, such that there were no significant differences compared to individuals with less pronounced tinnitus. Consistent with this, studies conducted in [13] found that tinnitus negatively affects directional hearing only in response to pure-tone stimuli. Thus, the training scheme is suitable for older CI users as well as those with strong tinnitus.
5 Conclusion and outlook
In this work we confirmed the feasibility and the benefit of a training scheme for directional hearing. However, the missing control group is a limitation of the study and should be considered in future projects in a larger cohort of CI users.
Due to the use of real-world stimuli in the proposed training scheme, we were not able to analyse the localization improvements in terms of interaural level and time differences, which would require stimuli with explicit low-pass or high-pass characteristics. This question as well as the effects of a prolonged or a more intensive training period warrant further evaluation.
Notes
Conference presentation
This contribution was presented at the 28th Annual Conference of the German Society of Audiology and published as an abstract [9].
Acknowledgements
The authors are grateful to all the CI patients that participated in the training as well as to the staff of the Cochlear Implant Center Ruhrgebiet and to Benjamin Lentz, M.Sc., Institute of Communication Acoustics, for discussions on the experimental design and statistical analysis.
Ethics statement
The study was approved by the ethics committee of the Medical Faculty of the Ruhr University Bochum, file no. 23-7754.
Funding
This work was supported by a grant from the Medical Faculty of the Ruhr University Bochum through its FoRUM (F1098-24) progam.
Competing interests
Christiane Völter has received reimbursement of scientific meeting participation fees and funding for research projects from MED-EL GmbH, Innsbruck, Austria. The other authors declare that they have no competing interests.
References
[1] Arndt S, Aschendorff A, Laszig R, Beck R, Schild C, Kroeger S, Ihorst G, Wesarg T. Comparison of pseudobinaural hearing to real binaural hearing rehabilitation after cochlear implantation in patients with unilateral deafness and tinnitus. Otol Neurotol. 2011 Jan;32(1):39-47. DOI: 10.1097/MAO.0b013e3181fcf271[2] Bates D, Mächler M, Bolker B, Walker S. Fitting Linear Mixed-Effects Models Using lme4. Journal of Statistical Software. 2015;67(1):1-48. DOI: 10.18637/jss.v067.i01
[3] Bernstein JG, Goupell MJ, Schuchman GI, Rivera AL, Brungart DS. Having Two Ears Facilitates the Perceptual Separation of Concurrent Talkers for Bilateral and Single-Sided Deaf Cochlear Implantees. Ear Hear. 2016;37(3):289-302. DOI: 10.1097/AUD.0000000000000284
[4] Blauert J. Spatial Hearing: The Psychophysics of Human Sound Localization. Revised ed. Cambridge, MA, London: MIT Press; 1996. DOI: 10.7551/mitpress/6391.001.0001
[5] Daher GS, Kocharyan A, Dillon MT, Carlson ML. Cochlear Implantation Outcomes in Adults With Single-Sided Deafness: A Systematic Review and Meta-analysis. Otol Neurotol. 2023 Apr;44(4):297-309. DOI: 10.1097/MAO.0000000000003833
[6] Dillon MT, Buss E, Anderson ML, King ER, Deres EJ, Buchman CA, Brown KD, Pillsbury HC. Cochlear Implantation in Cases of Unilateral Hearing Loss: Initial Localization Abilities. Ear Hear. 2017;38(5):611-9. DOI: 10.1097/AUD.0000000000000430
[7] Firszt JB, Reeder RM, Dwyer NY, Burton H, Holden LK. Localization training results in individuals with unilateral severe to profound hearing loss. Hear Res. 2015 Jan;319:48-55. DOI: 10.1016/j.heares.2014.11.005
[8] Gibbons JD, Chakraborti S. Nonparametric Statistical Inference. 5th ed. New York: Chapman and Hall/CRC; 2010. DOI: 10.1201/9781439896129
[9] Klatt WA, Oberländer K, Martin R, Völter C. Richtungshörtraining bei einseitig ertaubten CI-Trägern. In: Deutsche Gesellschaft für Audiologie e. V., editor. 28. Jahrestagung der Deutschen Gesellschaft für Audiologie. Oldenburg, 04.-06.03.2026. Düsseldorf: German Medical Science GMS Publishing House; 2026. Doc121. DOI: 10.3205/26dga121
[10] Kuk F, Keenan DM, Lau C, Crose B, Schumacher J. Evaluation of a localization training program for hearing impaired listeners. Ear Hear. 2014;35(6):652-66. DOI: 10.1097/AUD.0000000000000067
[11] Lentz B, Martin R, Weber L, Völter C. Development and First Evaluation of a Spatial Auditory Training Program for SSD Cochlear Implant Users. Otol Neurotol. 2025 Sep;46(8):909-17. DOI: 10.1097/MAO.0000000000004557
[12] Litovsky RY, Moua K, Godar S, Kan A, Misurelli SM, Lee DJ. Restoration of spatial hearing in adult cochlear implant users with single-sided deafness. Hear Res. 2019 Feb;372:69-79. DOI: 10.1016/j.heares.2018.04.004
[13] Long Y, Wang W, Liu J, Liu K, Gong S. The interference of tinnitus on sound localization was related to the type of stimulus. Front Neurosci. 2023;17:1077455. DOI: 10.3389/fnins.2023.1077455
[14] Ludwig AA, Meuret S, Battmer RD, Schönwiesner M, Fuchs M, Ernst A. Sound Localization in Single-Sided Deaf Participants Provided With a Cochlear Implant. Front Psychol. 2021;12:753339. DOI: 10.3389/fpsyg.2021.753339
[15] Schoen F, Mueller J, Helms J, Nopp P. Sound localization and sensitivity to interaural cues in bilateral users of the Med-El Combi 40/40+cochlear implant system. Otol Neurotol. 2005 May;26(3):429-37. DOI: 10.1097/01.mao.0000169772.16045.86
[16] Shim L, Lee J, Han JH, Jeon H, Hong SK, Lee HJ. Feasibility of Virtual Reality-Based Auditory Localization Training With Binaurally Recorded Auditory Stimuli for Patients With Single-Sided Deafness. Clin Exp Otorhinolaryngol. 2023 Aug;16(3):217-24. DOI: 10.21053/ceo.2023.00206
[17] Valzolgher C, Bouzaid S, Grenouillet S, Gatel J, Ratenet L, Murenu F, Verdelet G, Salemme R, Gaveau V, Coudert A, Hermann R, Truy E, Farnè A, Pavani F. Training spatial hearing in unilateral cochlear implant users through reaching to sounds in virtual reality. Eur Arch Otorhinolaryngol. 2023 Aug;280(8):3661-72. DOI: 10.1007/s00405-023-07886-1
[18] Van de Heyning P, Távora-Vieira D, Mertens G, Van Rompaey V, Rajan GP, Müller J, Hempel JM, Leander D, Polterauer D, Marx M, Usami SI, Kitoh R, Miyagawa M, Moteki H, Smilsky K, Baumgartner WD, Keintzel TG, Sprinzl GM, Wolf-Magele A, Arndt S, Wesarg T, Zirn S, Baumann U, Weissgerber T, Rader T, Hagen R, Kurz A, Rak K, Stokroos R, George E, Polo R, Medina MDM, Henkin Y, Hilly O, Ulanovski D, Rajeswaran R, Kameswaran M, Di Gregorio MF, Zernotti ME. Towards a Unified Testing Framework for Single-Sided Deafness Studies: A Consensus Paper. Audiol Neurootol. 2016;21(6):391-8. DOI: 10.1159/000455058
[19] van Heteren JAA, van Oorschot HD, Wendrich AW, Peters JPM, Rhebergen KS, Grolman W, Stokroos RJ, Smit AL. Sound Localization in Single-Sided Deafness; Outcomes of a Randomized Controlled Trial on the Comparison Between Cochlear Implantation, Bone Conduction Devices, and Contralateral Routing of Signals Hearing Aids. Trends Hear. 2024;28:23312165241287092. DOI: 10.1177/23312165241287092
[20] Wesarg T, Aschendorff A, Baumgaertel R, Böttcher J, De Coninck L, Dhooge I, Dierckx A, Klenzner T, Schörg P, Sprinzl G, Swinnen F, Verhaert N, Vermeiren A, Volpert S, Zarowsk A, Ernst A. Cochlear Implantation in Single-Sided Deafness and Asymmetric Hearing Loss: 12 Months Follow-up Results of a European Multicenter Evaluation. J Int Adv Otol. 2024 Jul;20(4):289-300. DOI: 10.5152/iao.2024.231457
[21] Zeitler DM, Dorman MF, Natale SJ, Loiselle L, Yost WA, Gifford RH. Sound Source Localization and Speech Understanding in Complex Listening Environments by Single-sided Deaf Listeners After Cochlear Implantation. Otol Neurotol. 2015 Sep;36(9):1467-71. DOI: 10.1097/MAO.0000000000000841

